Anti-Diabetic Drugs
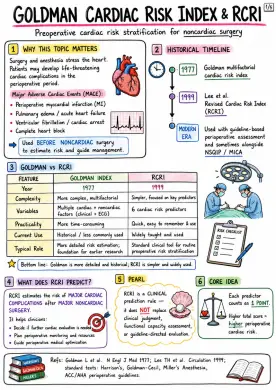
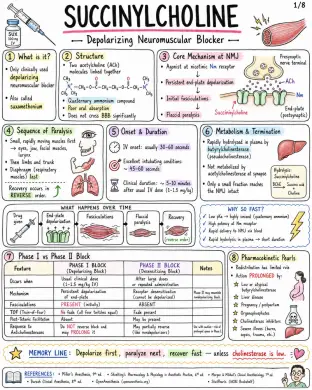
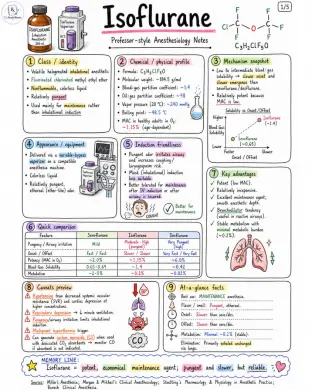
Image 1: Why This Topic Matters In Anesthesia: - Diabetic patients are common in OT/ICU. - Perioperative fasting alters glucose control. - Oral agents may need withholding to avoid hypoglycemia/drug interactions. - Insulin adjustment is crucial to maintain euglycemia perioperatively. - Both hypoglycemia and hyperglycemia increase morbidity & mortality. - Some drugs carry risk of lactic acidosis or euglycemic DKA – important in perioperative care. Mini-Index (What's Inside): - Overview, classification & glycemic targets - Biguanides (Metformin) - Sulfonylureas & meglitinides - Thiazolidinediones, alpha-glucosidase inhibitors & other older agents - DPP-4 inhibitors & GLP-1 receptor agonists - SGLT2 inhibitors & miscellaneous newer agents - Insulin preparations, regimens & delivery - Adverse effects, contraindications & important comparisons - Perioperative/anesthesia considerations, viva questions & references Learning Objectives: - Classify anti-diabetic drugs systematically. - Know mechanism of action, uses, adverse effects & contraindications. - Compare agents for efficacy, safety & special uses. - Understand perioperative (anesthesia) management principles. Quick Memory: - Think → Mechanism → Main uses → Adverse effects → Contraindications → Perioperative points Professor's Note: - For exams, always write classification first, then MOA, uses, adverse effects, contraindications, and perioperative relevance. Exam Strategy: - Classification - MOA - Uses - Adverse effects - Contraindications - Perioperative relevance Image 2: Diabetes Mellitus - Brief Context: - Chronic hyperglycemia due to defects in insulin secretion, insulin action, or both. - T1DM: absolute insulin deficiency due to β-cell destruction. - T2DM: insulin resistance with relative insulin deficiency. Therapeutic Goals: - HbA1c target for most adults: <7% (individualize) - Fasting plasma glucose: 80-130 mg/dL - 2-hour postprandial glucose: <180 mg/dL - Avoid hypoglycemia in all treatment plans. Classification of Anti-Diabetic Drugs: - Class 1: Insulin - Rapid-acting, Short-acting, Intermediate, Long-acting, Premixed analogs - Replaces endogenous insulin; promotes glucose uptake, suppresses hepatic glucose output. - Class 2: Biguanide - Metformin - Decreases hepatic gluconeogenesis; improves insulin sensitivity; ↓ intestinal glucose absorption. - Class 3: Sulfonylureas - Glimepiride, Gliclazide, Glipizide, Glyburide (Glibenclamide) - Stimulate pancreatic β-cells ↑ insulin secretion. - Class 4: Meglitinides - Repaglinide, Nateglinide - Short-acting secretagogues; stimulate β-cells ↑ insulin. - Class 5: Thiazolidinediones - Pioglitazone - PPAR-γ agonist ↑ insulin sensitivity in muscle & adipose tissue; ↓ hepatic glucose output. - Class 6: Alpha-Glucosidase Inhibitors - Acarbose, Miglitol, Voglibose - Inhibit intestinal α-glucosidases → delay carbohydrate digestion & absorption; ↓ postprandial glucose. - Class 7: DPP-4 Inhibitors - Sitagliptin, Vildagliptin, Saxagliptin, Linagliptin, Alogliptin - Inhibit DPP-4 ↑ endogenous GLP-1 & GIP → ↑ insulin secretion, ↓ glucagon. - Class 8: GLP-1 Receptor Agonists - Exenatide, Liraglutide, Dulaglutide, Semaglutide - GLP-1R agonism ↑ insulin, ↓ glucagon, delayed gastric emptying, ↓ satiety → weight loss. - Class 9: SGLT2 Inhibitors - Dapagliflozin, Empagliflozin, Canagliflozin - Inhibit SGLT2 in renal PCT ↑ glucosuria → ↓ plasma glucose; mild diuresis & natriuresis. - Class 10: Amylin Analog - Pramlintide - Amylin analog ↓ glucagon, gastric emptying, ↑ satiety → ↓ postprandial glucose & weight. - Class 11: Others - Colesevelam, Bromocriptine, Tirzepatide - Colesevelam: bile acid sequestrant; improves glycemia. - Bromocriptine: dopamine agonist; improves insulin sensitivity. - Tirzepatide: dual GIP/GLP-1 receptor agonist. Major Pathophysiologic Defects in T2DM & Where Drugs Act: - Liver: ↑ Hepatic glucose production - Metformin T2Ds Insulin - Pancreas: ↓ Insulin secretion - SU, Meglitinides DPP-4i, GLP-1 RA Insulin - Muscle Adipose: Insulin resistance - Metformin T2Ds SGLT2i - Gut: ↑ Carbohydrate absorption & incretin dysfunction - α-GI inhibitors DPP-4i GLP-1 RA - Kidney: ↑ Glucose reabsorption - SGLT2 inhibitors General Prescribing Principles: - Choose drugs based on: efficacy, hypoglycemia risk, weight effect, comorbidities (ASCVD, HF, CKD). - Consider patient factors: age, duration of diabetes, renal/hepatic function, cost & preferences. - Start low, go slow; titrate to target. - Prefer agents with proven CV/Renal benefit in appropriate patients. - Reassess regularly: efficacy, safety, adherence, side effects & goals. Professor's Exam Tip: - Always write classification first, then MOA, uses, adverse effects, contraindications, and perioperative relevance. Image 3: Mechanism of Action: - Activates AMPK - Hepatic gluconeogenesis - Intestinal glucose absorption - Peripheral insulin sensitivity - Does not stimulate insulin release Pharmacokinetics: - Oral - Not metabolized - Excreted unchanged by kidney - Half-life about 4-8 h - Use with meals to reduce GI upset Clinical Uses: - First-line therapy in T2DM - Prediabetes in selected patients - Obesity / insulin resistance - Polycystic ovary syndrome (PCOS) - Combination therapy with insulin or other agents Advantages: - No hypoglycemia when used alone - Weight neutral or modest loss - Improves insulin resistance - Low cost - Possible cardiovascular benefit Adverse Effects: - Nausea - Abdominal discomfort - Diarrhea - Metallic taste - Vitamin B12 deficiency (long-term use) - Rare: lactic acidosis Contraindications / Cautions: - Severe renal impairment (eGFR < 30 mL/min/1.73 m^2) - Acute kidney injury risk - Severe hypoxia / shock / sepsis - Severe liver disease - Alcoholism - Dehydration - Iodinated contrast-related situations Lactic Acidosis - Exam Pearl: - Very rare but serious - Risk factors: - Renal impairment - Hypoxia (CHF, shock, sepsis) - Liver disease / alcoholism - Dehydration - Advanced age - Concomitant nephrotoxic drugs Perioperative Relevance: - Usually withheld on the day of surgery or when fasting - Withhold around iodinated contrast or with renal dysfunction - Restart when renal function and oral intake are adequate - Monitor renal function Metformin vs. Sulfonylurea: - Metformin: - No weight gain (may cause modest loss) - Minimal risk of hypoglycemia - Sulfonylurea: - Causes hypoglycemia - Causes weight gain Image 4: Core Concept: - Both are insulin secretagogues – they stimulate pancreatic β-cells to release endogenous insulin. Classification: - Sulfonylureas - 1st Generation (mainly historical) - Tolbutamide - Chlorpropamide - 2nd Generation (widely used) - Glibenclamide (Glyburide) - Glipizide - Gliclazide - Glimepiride - Meglitinides - Repaglinide - Nateglinide Mechanism (Step-by-Step): - Bind SUR1 on pancreatic β-cell KATP channel - Channel closure - Depolarization - Ca2+ influx - Insulin release Comparison: Sulfonylureas vs Meglitinides: - Feature - Sulfonylureas - Onset: 30–60 min - Duration: Long (12-24 h) - Dosing relative to meals: Once or twice daily (not meal-timed) - Effect on postprandial glucose: Moderate - Renal issues: Caution in renal impairment - Hypoglycemia risk: Higher & prolonged - Feature - Meglitinides - Onset: 15–30 min (rapid) - Duration: Short (2-4 h) - Dosing relative to meals: Just before each main meal - Effect on postprandial glucose: Strong (better control) - Renal issues: Preferred in renal impairment (dose adj.) - Hypoglycemia risk: Lower & shorter Glucose-Lowering Effect vs Hypoglycemia Risk: - Sulfonylureas: strong effect but higher hypoglycemia risk - Meglitinides: strong PPG control with lower risk Uses: - Type 2 Diabetes Mellitus (T2DM) with residual β-cell function. - Meglitinides are especially useful for patients with irregular meal schedules or predominant postprandial hyperglycemia. Adverse Effects: - Hypoglycemia - Weight gain - Extra Notes: - Chlorpropamide → disulfiram-like reaction (with alcohol), SIADH. - Sulfa allergy caution (cross-reactivity). - Repaglinide interacts with gemfibrozil (↑ repaglinide levels → hypoglycemia). Contraindications: - Type 1 Diabetes Mellitus (T1DM) - Diabetic ketoacidosis (DKA) - Pregnancy (preference: insulin) - Severe hepatic disease - Patients at high risk of hypoglycemia (e.g., elderly, frail, malnourished) Exam Pearl: - Glibenclamide (glyburide) has the highest risk of hypoglycemia due to long duration. - Glimepiride and Gliclazide are commonly preferred (lower risk and better safety profile). Perioperative / Anesthesia Relevance: - Omit the morning dose on the day of surgery. - These agents can cause hypoglycemia during fasting and under anesthesia. - Monitor blood glucose perioperatively and manage as per protocol. Image 5: Thiazolidinediones (TZDs): - MOA: PPAR-γ agonist → ↑ insulin sensitivity in adipose tissue, muscle, liver - Uses: T2DM with insulin resistance - Advantages: durable effect, no hypoglycemia when used alone - Adverse effects: weight gain, edema, heart failure exacerbation, fractures, possible hepatotoxicity, anemia, bladder cancer concern with pioglitazone (debated; long-term caution) - Contraindications/Cautions: heart failure, active liver disease Alpha-Glucosidase Inhibitors: - Acarbose, Miglitol, Voglibose - MOA: Delay intestinal carbohydrate digestion/absorption by inhibiting alpha-glucosidase → mainly lowers postprandial glucose - Adverse effects: flatulence, abdominal discomfort, diarrhea Other Less Commonly Used Agents: - Colesevelam: bile acid sequestrant; modest glucose l